

20
Sep
Dehydration in endurance sports: risks to performance and how to manage it
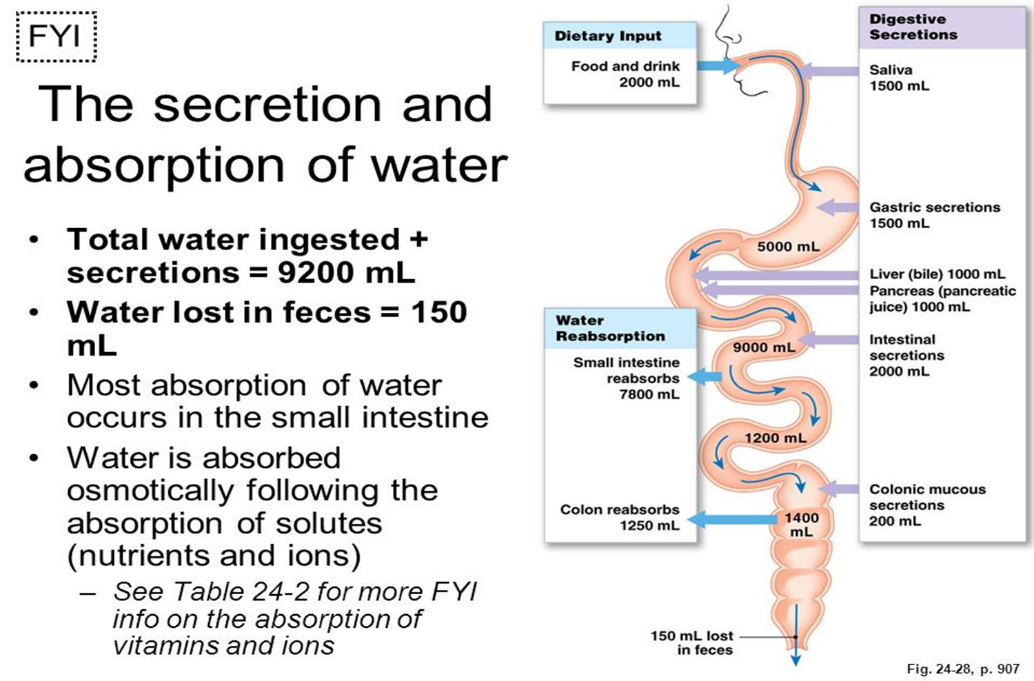
In a sedentary person, the daily exchange of water is about 2.5 litres (intake and output), but the liquids that actually circulate in the entire digestive system amount to about 9 litres. In an athlete, the quantities vary considerably due to an increase in outflow, mainly in the form of sweat. These losses must be adequately compensated for by an increase in intake.
The quantity of water to be replenished varies according to the individual characteristics, the intensity and quantity of muscular work and, above all, in relation to the climatic conditions.
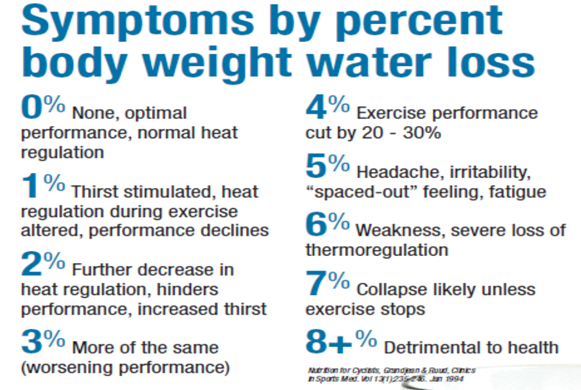
Broadly speaking, the water requirement of a person who performs physical activity is about 1 ml for each calorie of energy expenditure. If physical activity exceeds 2 hours, dehydration can reach up to 5% of body weight . This lack of fluids must be adequately and promptly rebalanced, otherwise it creates the conditions for a rapid deterioration in the athlete’s performance .
Some absurd sporting regulations prohibit the supply of water during the race, essential instead to avoid creating problems due to excessive loss of water, especially on hot and humid days, that recommendations are issued to take an additional amount of liquids before the exercise, not only during and after, favoring hypotonic or isotonic solutions.
Respect for the choice of hypo / isotonic solutions is necessary to avoid that a significant amount of pure water leads to the dilution of extracellular fluids causing, thanks to the action of the pituitary, the incretion of adiuretine with consequent elimination of excess fluids unpleasant consequences for an athlete.
Sometimes, despite the intake of drinks rich in salts, the athlete is unable to increase the absorption of Na because the thirst “signal” stimulates the absorption of liquids but is unable to determine the correct balance of electrolytes. This occurs mainly in untrained subjects and in particular climatic conditions.
Many professional athletes, accustomed to great exertion with conspicuous sweat profusions, develop the ability to produce electrolyte-poor sweat.
In general, the lack of fluids and salts, especially in humid heat conditions, is signaled by symptoms such as nausea, vomiting, dizziness and general fatigue, as well as a significant impairment in performance. If persisted, muscle cramps, mental apathy and convulsions may occur.
To correctly calculate the quantity of substances to be reintegrated, it is necessary to remember some concepts related to osmolarity.
Osmolarity : the volume of extracellular fluid is generally estimated at 0.255 l / kg of body weight. The main factor that regulates the distribution of body water between the extracellular (EC) and intracellular (IC) districts is the osmotic pressure of the liquids themselves. Osmotic pressure is defined as that pressure that exactly balances the movement of the solvent generated by the difference in solute concentration between 2 concentrations.
Per an ideal solute we have:
P.Osm = nRT / V dove n / V = moli / m3 = mmoli / liter
Always consider the difference:
Osmolality : mosmoles / l of solvent; Osmolarity: mosmoles / l of solution.
In dilute aqueous solutions of undissociated solutes, such as glucose, osmolarity = osmolality
When a solute dissociates (eg NaCl) it is necessary to take into account the increase in the number of particles (Na and Cl ions). Therefore, a 100 mmol aqueous NaCl solution has the same osmotic pressure as a 200 mmol glucose solution.
The osmotic pressure produced by substances with low PM (crystalloids) must not be confused with that determined by substances such as Protein (colloids), where the latter is called “oncotic pressure”.
Protein are relatively non-permeating anions, while other ions permeate more or less easily, which explains the differences in the concentrations of small ions on both sides of the capillary endothelium.
Plasma Protein contribute approximately 7.5% to the anionic concentration of plasma.
Therefore about 93% of the osmolality of plasma and interstitial liquids is attributable to electrolytes, in particular Na, Cl and HCO3-.
The real osmolality, however, is only 90 – 95% of the theoretical one calculated due to the deviations, by the solutes, of what are the ideal conditions, but these differences are not relevant from a functional point of view.
The various solutions to be considered isotonic or isosmotic with plasma must have an osmolality of 270 – 320 mosmoles / l of solvent.
The importance of a correct interpretation of osmolarity becomes fundamental in the preparation of a solution that must reintegrate energies and mineral salts in the athlete. First of all, it is necessary to identify the goal, that is, if you are aiming for a quick replenishment of the water or if you want a quick energy supply.
However, some old rules are always valid: it has been noted that some sugars have a “dragging” effect, ie solutions with dissolved the 4 main ions lost with sweat (Na, Cl, K and Mg) are absorbed more quickly, during transit in the intestinal lumen, if they are in the presence of some sugars.
An isotonic solution also guarantees a fast transit in the stomach, just slower than that of pure water.
TYPE AND VOLUME OF BEVERAGE TRANSITING THE STOMACH
IN 20 MINUTES
-
Type (% glucose)
Volume in ml
0 (pure water)
64
5
60
8
55
10
47
20
20
A hypertonic solution, that is, with an osmotic pressure higher than that of the plasma, remains longer in the stomach and, once it reaches the intestinal lumen, due to the high osmolarity, draws a quantity of liquids from the mucosa (theft of water). The subtraction of water damages the entire organism, worsening any dehydration, causing diarrhea and, in any case, limiting athletic performance.
Very frequently, dehydration is caused by improperly conducted weight loss. Athletes generally lose weight for three reasons:
- Fall into a specific weight category;
- Aesthetically better qualitative aspect;
- Improve Performance.
There are many doubts raised regarding the potential damage to health, caused by continuous weight loss, clearly greater perplexities, if not certainties, derive from the methods, mostly empirical, used to lose weight quickly, in these cases the main component of the loss of weight is the consequent DEHYDRATION.
Some physiological aspects should always be kept in mind: body water represents about 60 percent of the total body weight in an adult man. The amount of intracellular water (ICW) amounts to 2/3 of the total body water (66%), while the content of extracellular water (ECW) amounts to 1/3 of the total body water TBW (35%).
The blood plasma results to be 20-25 percent of the extracellular water while the remaining 75% to the interstitial compartment of the extracellular water: in the dehydration due to rapid weight loss both compartments are involved in the loss of water.
It has been estimated that the ICW compartment contributes 30-60 percent of the total fluid loss; the interstitial fluid for 30-60 percent of the total, and the VPS (Blood Plasma Volume) for 8-12 percent of the total (Mack & Nadel 1996).
Voluntary dehydration is probably the most used technique for the rapid weight loss mode, and also the most specific to producing large body water losses.
Fasting or lightning diets with a very low calorie content lead to significant weight losses where a very low energy intake inevitably leads to high losses of body water due to the degradation of glycogen and Protein, with the following repercussions on physiological functions and performance:
- Reduced improvement, no changes or possible reduction in muscle strength;
- Reduction of anaerobic Energy;
- Reduction in plasma and blood volume; increase in HR (heart rate) at rest and during sub-maximal work; decrease in systolic flow; reduction of work capacity.
- Reduced oxygen consumption.
- Imbalances in thermoregulation capable of decreasing stamina and increasing the risk of heat diseases during physical activity.
- Decreased blood supply to the kidneys and decreased renal filtration.
- Depletion of muscle glycogen and possible depletion of the hepatic one, with evident reduction of the resistance capacity of the muscle and of the body’s ability to maintain normal glycemic levels; increase in protein catabolism.
- Electrolyte depletion with consequent alteration of the muscle contraction capacity; coordination problems; cardiac arrhythmias.
Some useful data to reconsider the negativities of dehydration: with a rapid loss of body weight from 4.1 to 6.3%, a decrease in VPS was found from 1.4 to 14.8%.
In a study conducted on wrestling athletes, a loss of weight from 3.3% to 5.8% in the 3-5 days prior to the competition leads to a reduction in blood plasma of approximately 6.3%.
A loss of body fluids even of only 1% corresponds to a significant increase in body temperature, compared to an optimal hydration condition.
Per every liter of sweat that is produced, the HR for the same workload increases by 8 pulses * min-1 and cardiac output decreases by 1 L * min-1.
When dehydration in a period of rapid weight loss amounts to 4-5% of body mass, there is an evident decrease in work capacity and a reduction in many functions related to the athletic component, among these of particular importance the decrease in buffering capacity. muscle acidity, decrease in the lactate threshold.
An adequate water balance during physical activity is essential for optimizing cardiovascular and thermoregulatory functions.
At the beginning of physical exercise, water is transferred from the blood plasma (ECW) to the interstitial and intracellular spaces: the metabolites begin to accumulate in and around the muscle Fibre, the osmotic pressure in these sites is increasing and attracts water . Increasing muscle activity raises blood pressure with “extravasation” of water from the vascular compartment, often associated with an increase in sweating: in essence, from all these effects due to the increase in physical activity, the muscles acquire water at the expense of plasma volume.
On the other hand, the reduction in plasma volume results in:
- Reduction in blood pressure
- Reduction of blood flow to the epidermis
- Reduced blood flow to the muscles
These combined effects unfortunately seriously compromise sporting performance. One of the mechanisms involved derives from the fact that a rapid weight loss corresponds to a reduction in VPS, but the loss of electrolytes to the same extent as water is not allowed, consequently there is a change in the plasma osmolarity which increases (haemoconcentration) with relative increase of the concentration gradient.
The reduction in VPS results in a reduction in the global plasma mass followed by an increase in blood viscosity which, in turn, causes negative effects on cardiovascular function, including: the reduction in Volume / Minute (cardiac output); reduction of systolic discharge (by 25-30%); increased heart rate attributed to reduced systolic discharge. The consequent increase in heart rate is not enough to compensate for a decreased systolic shock, which results in a reduction in cardiac output.
The reduction of cardiac capacity reduces the overall effectiveness of oxygen transport, producing metabolic disturbances in the active muscle that will work in anaerobiosis, accelerating the consumption of glycogen stores.
Even a modest dehydration (1% of the CP) caused by sweating during exercise can increase cardiovascular work by increasing the HR and reducing the body’s thermoregulatory capacity.
Let’s recap the consequences of dehydration resulting from rapid weight loss:
- Decreased volume and blood pressure;
- Reduction of the sub-maximal and maximal systolic discharge volume and of the maximum cardiac output (Volume / minute);
- Decreased blood perfusion to the kidneys, and through the kidneys;
- Increase in sub-maximal HR;
- Reduction of aerobic and anaerobic capacities;
- Decline in performance;
- Significant impediment to thermoregulation.
- Loss of Liquids;
- Decrease of alkali reserves, at rest.
Athletes trying to obtain a low body weight with very drastic diets therefore obtain a prevalent drop in body fluids, therefore on the basis of the previous indications it is natural to draw general conclusions on the action exerted by the aforementioned Weight Loss on athletic performance, as is certain that a reduction in lean mass leads to a decrease in the organism’s capacity for strength.
Strength reduction should be taken more seriously as Energy is a prerequisite for success, and this conflicts with the theory that weight reduction allows the athlete to gain a real competitive edge.
Certainly not secondary are the health implications highlighted above, to which is added a concrete alteration of the thermoregulation mechanism. Sawka in 1992 concluded in a review that dehydration causes a huge storage of heat that is not dissipated by the body (deep body temperature increase), thus reducing the tolerance to heat stress. This is the result of the quantitative reductions in sweat and blood circulation.
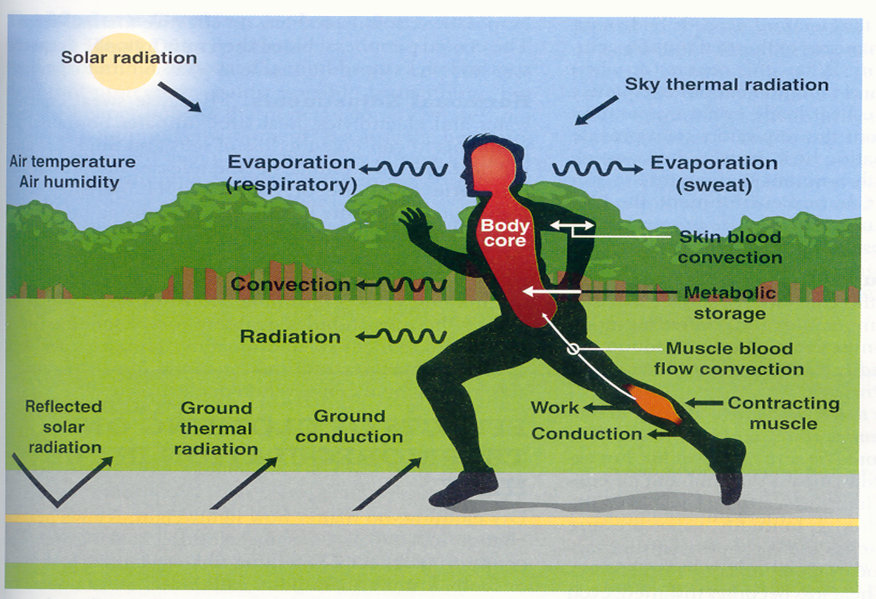
Uniformly with the reduction of blood circulation, there is a relative reduced mobility of the subcutaneous peripheral blood circulation which, among other things, has the task of cooling the skin and therefore the deep body temperature, generating difficulties for the maintenance of venous blood pressure and a adequate systolic range.
Excessive sweating and / or urinary urination could also be a consequence of the large loss of electrolytes, which could have serious repercussions such as cardiac dysarrhythmias, although Costill observed that this uniform loss of electrolytes, although considerable, derives mainly from the ECW compartment and therefore, the loss of ions by sweating and urinating has little effect on the K + ion content in the muscle cell.
Unfortunately, there are still several difficulties for a possible precise and detailed management regarding the prevention of excessive sweating:
- You do not sweat with the same intensity, neither between different subjects, nor in apparently the same conditions
- There is no constancy in the ionic composition of sweat
- No reliable predictive index emerged on the amount of fluids that an athlete will lose (urine osmolarity, sweat, programmed pre-hydration): environmental and individual variables are imponderable
![]()
What considerations can be drawn to counteract dehydration mainly dependent on rapid and excessive weight loss or in situations of difficult environmental conditions (humid heat) in which physical exercise is performed?
First of all, consider that the water absorption mechanisms in the intestinal lumen associate and modulate the absorption of nutrients thanks to the co-transport with some electrolytes by exploiting the relative channels, from which the study and formulation of appropriate solutions for a correct and complete hydration. Here are some fundamental points that must be considered in order to contain and / or avoid the negatives.
-
- Osmolarity and type of carbohydrates do not adversely affect gastric emptying for CHO concentrations up to 6%
- Volume more important than temperature in regulating gastric emptying
Shi et al. Int J Sports Nutr Exer Met 2000
- There are “active transporters” for many carbohydrates in the intestine. The presence of different carbohydrates in drinks therefore improves liquid portion absorption.
- The rate of intestinal absorption is influenced by: osmolality, type of Carbohydrates, number of Carbohydrates
- The impact of the “CHO number” factor is greater than the “osmolarity” factor
“C. Gisolfi legagy” 2001 ACSM Annual Meeting
- Solutions that contain different carbohydrates (therefore more than one) determine a greater uptake of water in the intestine.
(McArdle, Katch & Katch, Sports & Exercise Nutrition)
The addition of a small amount of sodium helps to maintain the plasma concentration of sodium, and thus reduce the production of urine and support the stimulus of thirst
(McArdle, Katch & Katch, Sports & Exercise Nutrition)
The volume of liquids to be taken must go from 50 to 70% higher than the losses
(ACSM Position Stand 2007)
BIBLIOGRAPHY
McARDLE W. D, KATCH F. I., KATCH V. L. “Fisiologia applicata allo SPORT”. Casa Editrice Ambrosiana, Milano, 1998.
OPPLIGER R. A., CASE H. S., HORSWILL C. A. et al. “La perdita di peso nei lottatori“, posizione ufficiale American College of Sports Medicine. Medicine and Science in Sports and Exercise. Vol. 28, N°2. 1996
ROEMMICH J. N., SINNING W. E. “Weight loss and wrestling training: effects o nutrition, maturation, body composition and strength”. Journal of Applied Physiology 82 : 1751-1759, 1997.
TIMPMANN S., OOPIK V. “L’ influenza della riduzione del peso corporeo sulla prestazione nello sport da combattimento“. Athlon 10/2005, 1-2/2006.
WILMORE J. H. “Weight Category Sports“; Parte 4, Cap. 49, in MAUGHAN R.J. “Nutrition in Sport“ , Volume VII of the Encyclopaedia of Sports Medicine, in collaboration with the International Federation of Sports Medicine. Blackwell Science, 2002.
Damir Zubac, Armin Paravlic, Reid Reale, Igor Jelaska, Shawnda A Morrison, Vladimir IvancevEur J Nutr. 2019 Mar;58(2):497-514. Fluid balance and hydration status in combat sport Olympic athletes: a systematic review with meta-analysis of controlled and uncontrolled studies.
Shirreffs SM et al. 2005, The sweating response of elite professional soccer players to training in the heat. Int. J. Sport. Med. 26 (2): 90-5.
Maughan, R. 2006. Guidelines for replacing fluid and CHO during exercice. In: Clinical sport nutrition-McGraw Hill.
R. J. Maughan, S. M. Shirreffs; Scand J Med Sci Sports 2010: 20 (Suppl. 2): 59–69. Development of hydration strategies to optimize performance for athletes in high-intensity sports and in sports with repeated intense efforts.
N.A. Masento, M. Golightly , D.T. Field, L.T. Butler and C.M. van Reekum; British journal of nutrition, January 2014, Effects of hydration status on cognitive performance and mood.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}